
With total hip arthroplasty, one of the main objectives is to provide a stable hip by restoring joint biomechanics. Failure to achieve this goal results in dislocation and may happen regardless of surgical approach.1 Dislocation after THA is the most common cause for revision hip surgery in the United States.2 Proper component position and soft tissue tension must be achieved during THA to reduce the risk of dislocation.3
This content is sponsored by Medacta.
Intraoperative instability during THA can be addressed by proper restoration of femoral offset. Leg-length equality and acetabular component position are also fundamental considerations in THA for patient satisfaction and prevention of dislocation.4 Patients with spinal deformities and younger, more active patients, create higher demands on implant components needed to improve functional outcomes and avoid dislocation.
This article discusses femoral and acetabular implant selection and how they can optimize offset restoration and improve joint stability with the goal of reducing the risk of dislocation.
Femoral Offset & Leg-length Equality
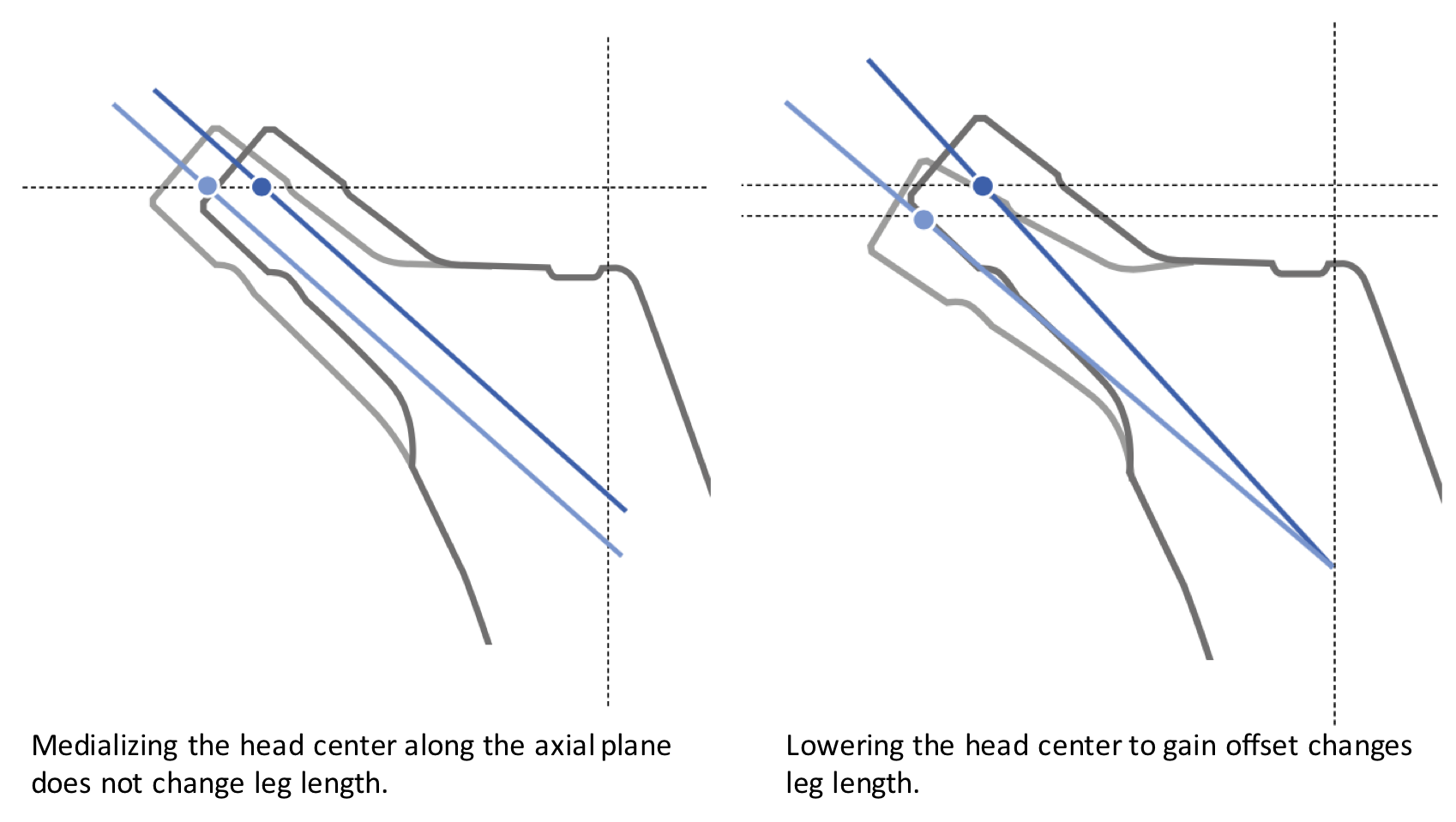
One of the differentiating factors of femoral hip stem implants is how they address offset. Femoral stem implants usually offer two offset options to address soft tissue tension. Most of the femoral stem systems medialize the head center along the axial plane, which tightens the hip joint without changing leg length. The amount of offset between a standard and lateralized offset neck normally ranges from 6 mm to 8 mm.
Some femoral stem systems lower the head center when offset is added. This changes the leg length and can complicate the intraoperative decision-making process. Other systems may offer a reduced neck option or coxa vara neck option. These options will also shorten the leg and make the intraoperative decisionmaking process more complex. Leg-length discrepancy in these situations is a major concern in terms of patient satisfaction.
While two offset options provide good intraoperative flexibility to restore hip joint biomechanics, there are cases where femoral offset could be compromised. The standard option may be a bit too loose but adding 8 mm of offset may make the joint a bit too tight. When this is the case, less than optimal tensioning may occur.
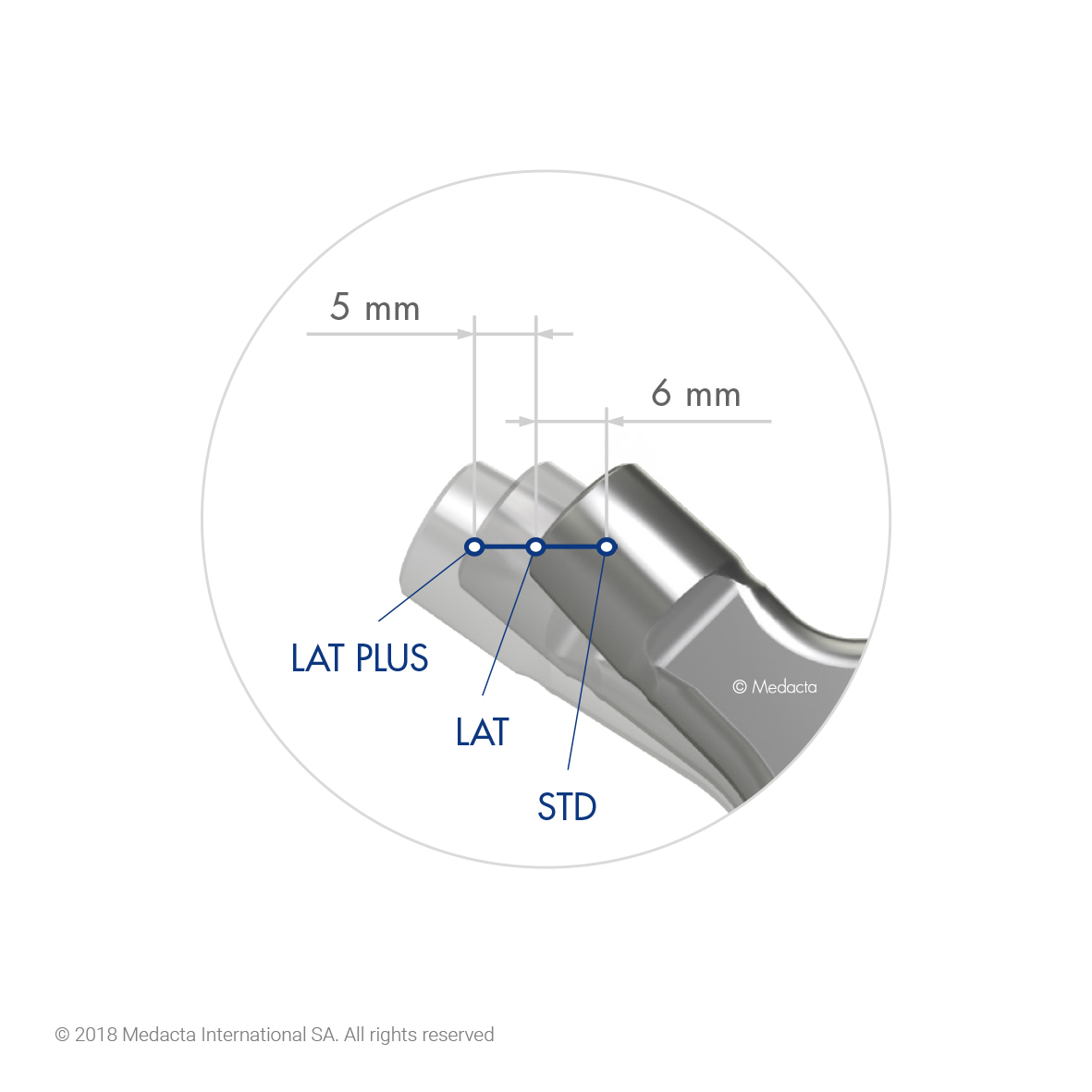
The MasterLoc™ Hip System from Medacta may provide the most comprehensive and straight-forward solution to addressing soft tissue tension. The MasterLoc System offers three offset options within an 11 mm range that do not change leg length. The standard version has less offset to accommodate smaller patients who may have less femoral offset. A lateralized version adds 6 mm of direct offset that does not change leg length. For patients that need more femoral offset, the lateralized plus option is a third offset alternative, which provides an additional 5 mm of offset that does not change leg length. MasterLoc has an unprecedented offset offering that delivers the most intraoperative choices to dialin femoral offset without compromising leg length.
 Ed Stolarski, MD: Patients expectations following total hip replacement have become increasingly more demanding. Return to a pain free lifestyle with no limitations and equal leg lengths are considered the "norm." Meeting these expectations is dependent on the approach as well as reestablishment of the patients' native biomechanics. Patients' leg length and offset should not be at the mercy of limited stem options including offset.
Ed Stolarski, MD: Patients expectations following total hip replacement have become increasingly more demanding. Return to a pain free lifestyle with no limitations and equal leg lengths are considered the "norm." Meeting these expectations is dependent on the approach as well as reestablishment of the patients' native biomechanics. Patients' leg length and offset should not be at the mercy of limited stem options including offset.
The MasterLoc stem gives me incredible versatility with three offset options within an 11 mm range. Whether it is avoiding increasing native offset of a valgus DDH neck or matching the most extreme varus offset, the MasterLoc stem allows for recreating that patient's native biomechanics. This reduces trochanteric bursitis in the DDH patient and avoids increasing leg lengthening for stability in those patients with significant offset. Another nice option is having the ability to go to the next level of offset in the patient whose operative limb is long or equal preop. I can make them equal under flouro and clinically, check stability. If unstable, I can add some offset instead of length. Ihave also been impressed by the uniform leg length as you increase offset, overall leg length does not change. It's a pure lateral move.
Lastly, I have used many flat, wedged taper stems and have always been challenged by the broach implant mismatch. The stem frequently sits proud compared to broach. I can honestly say that problem is virtuallyeliminated with the MasterLoc Hip System. The matched tolerance between the broach and the final implant is incredibly refreshing.
Acetabular Cup Positioning
Proper cup positioning is important to joint stability, function and reduction of polyethylene wear. Customary practice is to position the acetabular component in what is considered the "safe zone" of 15 ± 10 degrees of anteversion and 40 ± 10 degrees of inclination.5
Spinal deformities and subsequent spinal fusion along with degenerative diskdisease can increase the risk for dislocation due to spinal stiffness and can narrow the safe zone in regards to acetabular component positioning.6 Recently, this topic has gained more attention in the orthopedic community along with what may be the best means to treat patients with fixed spinopelvic alignment who need a total hip replacement. It has been suggested that surgeons should consider implant design options, such as large diameter or dual mobility bearings, to improve hip stability in patients with fixed spinopelvic alignment as they may be at higher risk of dislocation.7
Acetabular implant selection must also be considered for young and active patients who have higher activity levels that may demand greater range of motion. Larger diameter femoral heads improve hip joint stability by providing a larger jump distance before dislocation and increased ROM prior to impingement that can lead to lever-out dislocation.8
Double mobility acetabular components were introduced in France in the 1970s to reduce the risk of THA dislocation in patients undergoing primary THA. Double mobility components increase the headneck ratio and increase the arc of motion before impingement.9,10 In recent years, double mobility cups have gained wider acceptance in the United States to address joint instability in primary and revision THA. The addition of highly crosslinked polyethylene to double mobility implants has provided improved polyethylene wear characteristics, making it a preferred option for younger, active patients.11

Double mobility cups can take the form of monoblock cups or modular cups with hard-bearing inserts. The monoblock version provides a greater ROM and larger jump distance than the modular version. The modular version can allow for screw holes while providing secondary fixation that may be a benefit in lesser bone quality. However, some concerns of higher levels of metal ions have been reported with modular double mobility cups when dissimilar metals are mated to create the hard-bearing cup.12,13

The Mpact® DM from Medacta is a hemispherical, monoblock double mobility cup. It features a Mectagrip coating that has a high coefficient of friction for initial stability.14 The Mectagrip coating has open pores up to 350 µm in dimension that offers a favorable environment for bone growth leading to long term fixation.15, 16, 17, 18, 19 The articulating liner is HIGHCROSS polyethylene that provides a low wear bearing surface. The HIGHCROSS liner can be combined with a BIOLOX delta ceramic femoral head for younger, active patients.
 Rajeev Jain, MD: The Mpact Double Mobility Cup has become an integral part of my hip implant armamentarium to address patients who have a high risk of dislocation. Let me elaborate on some indications where I like to have the Mpact DM at my disposal.
Rajeev Jain, MD: The Mpact Double Mobility Cup has become an integral part of my hip implant armamentarium to address patients who have a high risk of dislocation. Let me elaborate on some indications where I like to have the Mpact DM at my disposal.
I have found that the effect of spinopelvic mobility challenges traditional thinking on acetabular component positioning. The traditional safe zone for acetabular component inclination and anteversion, as proposed by Lewinnek, may need to be reconsidered in some patients.5 For example, patients with stiff hips, limited spinopelvic motion, have the greatest risk for dislocation. It is in these situations that I like to increase my "safe zone" by using the Mpact DM double mobility cup. The onepiece Mpact DM cup allows me a femoral head that is 8 mm smaller than the shell size. For example, a 54 mm cup allows for a 46 mm double articulating femoral head.
Displaced femoral neck fractures treated with total hip arthroplasty have been associated with higher dislocation rates. There are many potential factors that can lead to instability, including an inability to evaluate the preexisting spinopelvic mobility. In these patients, I find the Mpact DM cup to be invaluable. In addition, I find that the high coefficient of friction of the plasma spray coating of the Mpact cup really grabs the acetabulum when implanting, even in these osteoporotic hip fracture patients.
Patients with CDD tend to lack functional anteversion that contributes to posterior hip
dislocation, because there is less posterior coverage of the acetabular component to stabilize the femoral head in sitting position.7 Besides maximizing the size of the articulating femoral head, the Mpact DM has a 5 degree raise on the shell that I can position posterior for additional head coverage for these circumstances.
Finally, younger patients suffering from hip arthritis who still participate in martial arts, gymnastics and dance refuse to give up their activities. The Mpact DM affords increased range of motion to accommodate these activities.
Your choice of implants can improve functional outcomes and reduce the risk of dislocation. Femoral stem implants that maximize your options to restore femoral offset without changing leg length can optimize hip joint biomechanics. For certain patient indications, a double mobility cup that increases the "safe zone" by providing a larger jump height and greater ROM can reduce the risk of dislocation.
References:
1. Kwon MS, et al. Does surgical approach affect total hip arthroplasty dislocation rates? Clin Orthop Relat Res. 2006;447:34–38.
2. Gwam CU, et al. Current epidemiology of revision total hip arthroplasty in the United States: National Inpatient Sample 2009 to 2013. J Arthroplasty 2017;32:2088e92. https://doi.org/10.1016/j.arth.2017.02.046.
3. Forde B., et al. Restoring femoral offset is the most important technical factor in preventing total hip arthroplasty dislocation. Journal of Orthopaedics 15 (2018) 131-133
4. M.M. Innmann et al. Additive influence of hip offset and leg length reconstruction on postoperative improvement in clinical outcome after total hip arthroplasty. The Journal of Arthroplasty 33 (2018) 156-161
5. Lewinnek GE, et al. Dislocations after total hipreplacement arthroplasties. J Bone Joint Surg Am 1978;60:217-20.
6. Buckland AJ, et al. Dislocation of a primary total hip arthroplasty is more common in patients with a lumbar spinal fusion. Bone Joint J 2017;99-B: 585-91.
7. C.I. Esposito et al. Total hip arthroplasty patients with fixed spinopelvic alignment are at higher risk of hip dislocation. J Arthroplasty article in press (2017) 1-6
8. Burroughs BR, et al. Range of motion and stability in total hip arthroplasty with 28-, 32-, 38-, and 44-mm femoral head sizes. J Arthroplasty 2005, 20(1):11–19
9. Heffernan C, et al. Does dual-mobility cup geometry affect posterior horizontal dislocation distance? Clin Orthop Relat Res 2014;472:1535-44
10. D'Apuzzo MR, et al. Relative head size increase using an anatomic dual mobility hip Prosthesis compared to traditional hip arthroplasty: impact on hip stability. J Arthroplasty 2014;29:1854-6
11. Epinette JA, et al. Early experience with dual mobility acetabular systems featuring highly crosslinked polyethylene liners for primary hip arthroplasty in patients under fifty-five years of age: an international multi-centre preliminary study. Int Orthop 2016
12. Ko LJ, et al. Serum metal ion levels following total hip arthroplasty with modular dual mobility components. J Arthroplasty. 31 (2016) 186–189
13. Nam D. Metal ion levels in young, active patients receiving a modular, dual mobility total hip arthroplasty. J Arthroplasty 32 (2017) 1581-1585
14. Friction testing of the Mpact and Versafitcup coating samples. Data on file Medacta.
15. Robotti P, et al. Macroporous titanium coatings , by thermal plasma spray. ITSC 2013, International Thermal Spray Conference, May 13 –15, 2013, Busan, Korea.
16. Biemond JE, et al, In vivo assessment of bone ingrowth potential of 3-dimensional E-beam produced implant surfaces and the effect of additional treatments by acid-etching and Hydroxyapatite coating. J Biomat Appl, published on line January 27, 2011, 0885328210391495.
17. Ferro de Godoy R., et al., In vivo evaluation of titanium macro-porous structures manufactured through an innovative powder metallurgy approach. Proceedings CM XIII: Bone Fixation, Repair & Regeneration, June 24–26, 2012, Davos, Switzerland.
18. Goodship A, et al. In-vivo assessment of the ingrowth potential of engineered surface topographies produced by spark plasma sintering, Proceedings 9th World Biomaterial Congress, June 1-5, 2012, Chengdu, China.
19. Data on file Medacta