
 Gastroesophageal reflux disease impacts many people in the United States and traditional treatment has shown varying degrees of success.
Gastroesophageal reflux disease impacts many people in the United States and traditional treatment has shown varying degrees of success. "In the field of reflux today, which is an increasingly diagnosed disease, there are upwards of 50 million people who suffer daily from their symptoms . and are dependent on medication for their treatment," says Mark Noar, MD, head gastroenterologist at The Endoscopy Center in Towson, Md. "Unfortunately, many aren't able to control their GERD symptoms. People who are prescribed medication aren't satisfied because they have to take pills every day and change their normal daily lifestyle, including having to watch their diets. There are interventional procedures that have had varying results. Stretta is different because the procedure addresses the primary problem that leads to the disease."
Dr. Noar discusses how the Stretta procedure is the safe and cost-effective treatment physicians and patients are looking for, and how ambulatory surgery centers and endoscopy centers can easily incorporate it into their schedules.
Q: How does the Stretta procedure fit into the current treatment pathway for GERD?
Dr. Mark Noar: Reflux is caused from too many relaxations of the lower esophageal sphincter which is in effect a guardian muscle against reflux. Everyone refluxes, but it's a question of how often and how much they reflux and what is the individual's sensitivity to the type of material that is being refluxed. If we can control that, we can have an impact on patients who suffer from uncomfortable reflux symptoms. We can improve the quality of life and limit the cost of medications as well as the potential risk of cancer. From my experience with Stretta, I believe it addresses all of these issues..
There are about 20 million reflux sufferers who don't respond to medication, no matter how many doses they take, and others who experience significant side effects. As we know the chronic use of these proton pump inhibitors can potentially alter the magnesium level, contribute to bone fractures and demineralization, and that chronic use could be associated with increased infections and even acute coronary artery syndrome.
Some patients might not be candidates for other interventional procedures because they've had issues such as a previous gastric bypass or bariatric surgery, and there are other underlying medical conditions preventing people from undergoing surgery. All these patients could undergo and potentially benefit from the Stretta procedure.
Q: In your experience, how successful is the procedure?
MN: We have seen a 92 percent initial success rate with Stretta. We have also been able to help patients with laryngeal or pulmonary symptoms, including sleep apnea, often eliminating their need for CPAP. In a certain subset of patients with sleep apnea, that don't present with typical reflux symptoms, they have been very responsive to the Stretta procedure because we are attacking the primary cause, which is too much reflux taking place too often into the throat or bronchial passages.
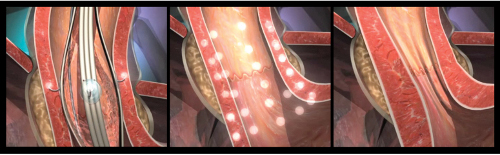
The procedure causes an increase in muscle fiber bundles as well as the amount of muscle in each bundle. The sphincter gets thicker and stronger, with a reduction in compliance and therefore opens less often. It's that reduction in the number of transient lower esophageal reflux relaxations that occurs that is important.
The device is extremely safe and we've seen a complication rate of essentially zero. The only symptom that patients might experience is chest discomfort for a few days, and they might require some pain medication. They are able to return to regular activities the next day. This procedure has been around for 13 years and more than 32 peer reviewed studies show patients are satisfied, can eliminate or significantly reduce medication usage and don't experience symptoms even 10 years after the procedure.
Q: Is this a procedure that would be safe in the ambulatory surgery center setting?
MN: These are procedures I perform in an outpatient ASC or endoscopy center. They are done with standard sedation. The entire procedure time is 20 to 25 minutes, with the actual Stretta portion taking only 14 minutes. It works extremely well in the ASC and that helps to control costs. There is already good research showing the safety records in the independent centers are better than hospitals, and we have the added benefit of working in a specialized environment.
How the procedure fits into the ASC is important. Not only are there the facility charges for having the procedure done there, but the patients require a number of pre-procedural diagnostics done that can positively impact the ASC's cash flow. They need various motility studies, acid reflux measurements, and esophageal motility impedance. This can be an effective business model for a center that decides to concentrate on reflux and ancillary procedures.
Q: What does it take for physicians to adopt this into their practice?
MN: The company that sells the device has an extensive array of educational materials that are available to the physicians that make the didactic portion and understanding about the procedure very easy. This does not require more equipment than would be present in a standard endoscopy suite or ASC performing endoscopy. The only additional requirement is the Stretta generator, which is small and mounts on a standard IV pole.
The procedure right now has a level 1 CPT code assigned to it and has had for many years. Up to two years ago, we had to fight for every case to be covered, but today Medicare is paying for them in many localities and we have other insurers on board, More are expected immediately with the release of the long term 10-year data showing the procedure is safe and very effective even after 10 years. It's getting easier to achieve coverage almost by the month, and we are seeing less resistance on the part of insurers.
Q: What are the potential complications associated with the procedure?
MN: We've done a lot of research looking on this procedure. There are a lot of nerve structures in this area and any time we use a new device we want to be sure it won't cause any damage. For instance if there was damage to the vagus nerve, there would be a worsening of stomach emptying. In fact just the opposite was proved in a published 2007 study showing that patients with gastroparesis and reflux were able to normalize emptying after Stretta. It improves gastric motility by keeping the lower esophageal sphincter closed when it's supposed to be closed, therefore allowing food to remain in the lower stomach where it can be pushed into the intestine by normal gastric contractions.
Another question arose about whether it would cause loss of sensation in the esophagus. There are studies looking at this issue and found the improvement in symptoms is related to a decrease in acid refluxing into the esophagus and not associated with sensory denervation. More simply explained, if I were accidentally to cut a sensory nerve that controls sensation to a finger, it would immediately become numb. But the Stretta procedure doesn't work that way and patients continue to have the sensation of reflux for days or weeks, until the acid is controlled and they improve.
There was also a concern that the device would cause scarring and physical restriction, but this is prevented by the Sretta generator that is extremely sensitive and set to eliminate these issues. The needle won't heat to a point where destruction would take place. Though it was unlikely that could happen, it was important to prove whether scarring was an issue. A study performed in Europe, employed Viagra which is a potent drug that relaxes the sphincter, and it showed patients had no scarring because the sphincter wouldn't have been able to relax otherwise.
Q: Healthcare dollars are becoming scarcer. Is this treatment cost-effective?
MN: We all know there is a finite number of healthcare dollars, so anything we can do to help save money is very important. Statistics published on the cost of GERD show that medication is nearly $1,000 per year per patient. The socioeconomic impact cost to the US healthcare system of GERD is $9,444 per year per patient,, including physician visits, increased tests and days missed from work. This makes GERD number three following asthma and diabetes. Considering that the all-in costs of Stretta is less than $3,000, this suggests a positive ROI to the healthcare system in 90 days. If we can stop reflux in an individual, we can stop that cost to society, which is an important factor.
Q: Do you think the Stretta procedure will become more widely adopted over the next few years?
MN: The surgeons are already strong adopters of this technology and many gastroenterologists are looking at it favorably. Patient selection becomes very important, but with proper patient selection it's very effective. There isn't a day that goes by where former Stretta patients come to see me, following up on other illnesses, and they are so excited because their reflux is controlled and they aren't taking medications. It becomes rewarding on another level for physicians.
However, I think if every gastroenterologist in the country would do the Stretta procedure every day in the classic reflux patent alone, they would barely scratch the surface for every patient who needs it. Considering that if you look at the patients with chronic cough and voice problems, as well as the new data now suggesting that in patients with COPD, asthma and sleep apnea sufferers, at least 50 percent of the patients have a significant reflux component, these patients too will be significantly impacted by the procedure. That's a patient population that until now has been largely untouched.
More Articles on Gastroenterology:
5 Recent GI Center Openings, Plans & Expansions
Have Gastroenterologists Stopped Taking Medicare?
9 Endoscopy Centers Receive 2012/2013 APEX Quality Award